Excellent Practices
Programme Structure
Practice Category: Patients
Centre: Cancer Research UK Cambridge Centre

Ken Seamon
kenneth.seamon@cruk.cam.ac.uk

Challenge which the practice addresses
Many Cancer Centres struggle to gain coherence in their organisational structures to integrate research and clinical care, and to maximise their opportunities. Comprehensive Cancer Centres with high volumes and breadth of research wish to preserve the ‘bottom up’ innovative power of research, and yet need to establish a clear structure to bring scientists into focused and resourced collaborations with clinicians and patients on more than an ‘ad hoc’ basis. Some centres attempt this by defining ‘Themes’ for both science and clinical excellence, but often these lack the organisational rigour or resource to be fully effective.
Solution
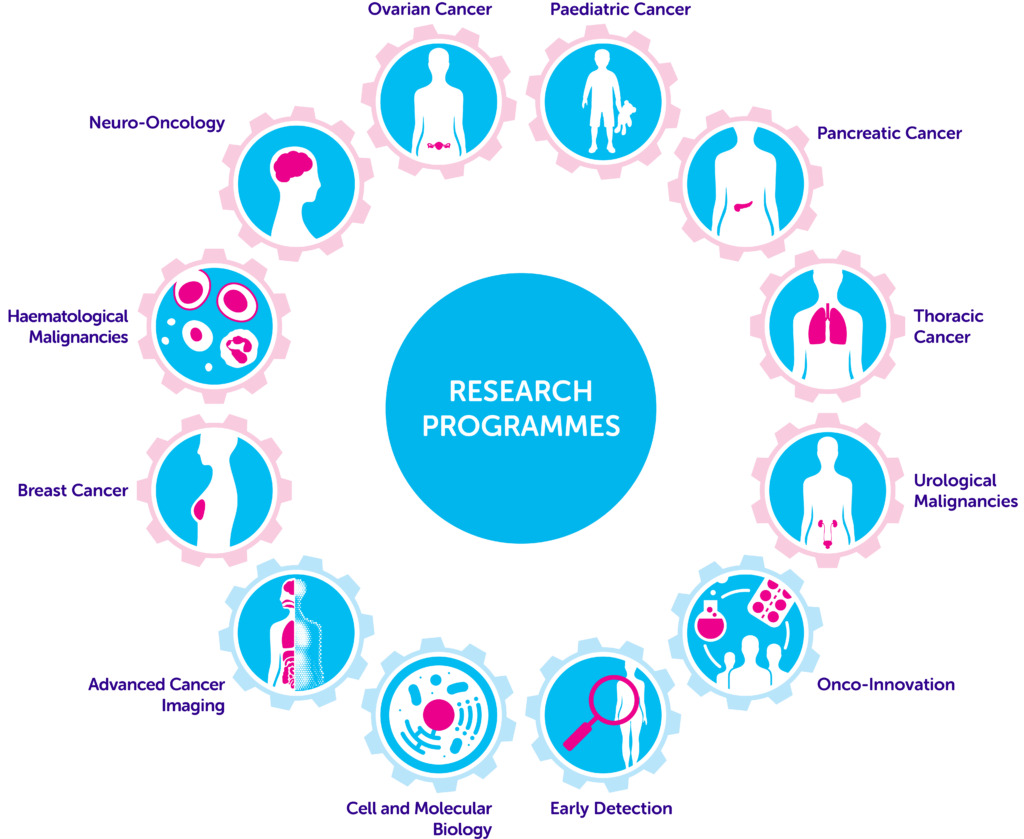
In the Cancer Research UK Cambridge Centre we established a Programme Structure in 2015. At that time we found through our individual membership register that there were approximately 600 scientific Group Leaders, PIs on clinical studies, and clinical consultants (surgeons, oncologists, radiologists, haemato oncologists and pathologists) working wholly or partly on cancer. Each was asked to align themselves with one of the 12 programmes established (see Figure 1) – 8 disease-specific, and 4 discipline-focussed. Two leaders were chosen for each programme (one a scientist; one a clinician) and a full- or part-time Programme Manager was appointed to each programme to manage and facilitate projects and collaborations. Programme sizes in terms of membership range from 40 to around 80. Budgets are delegated to each programme to grow the programme – to be utilised mainly for staff salaries, consumables, and pump priming grants to be offered for innovation for two or more groups working together across departments. Performance of each programme is monitored by the Director of the Centre, and the Executive Committee (comprising all Programme Leads) – introducing constructive challenge on strategy and performance, academic output, and clinical impact.
Impact
The impact of the programme structure is measured each year in reports to Cancer Research UK and the University of Cambridge. Constructive advice and critique is also offered by the International Scientific Advisory Board which visits the Centre in depth every 2 years. A major quinquennial review is also performed by Cancer Research UK on the centre activities and output.
Whilst a counterfactual controlled trial covering 2015-2021 is impossible, the following are highlights of the outputs and impacts of the programmatic approach to integrated science and clinical care in Cambridge:
- Quantity and quality of academic research outputs grew from 500 primary papers [125 impact factor >10] in 2016/17; to >750 primary papers [235 impact factor >10] in 2020/21.
- Clinical Trials: the Centre has consistently been in the top 5 recruiting hospitals in the UK, enrolling more than 7,800 patients in 230 prospective interventional trials in 5 years (26% of new patients on average).
- Membership: has increased from 607 scientists and clinicians in 2016/17, to 1,059 in 2020/21.
- Grants: major grants won in Early Detection; Precision Medicine; 3-D tumour mapping.
- Early Detection: invention of the CytospongeTM and lab test to rapidly detect Barrett’s Oesophagus as a non-invasive and cost-effective alternative to endoscopy (being rolled out as standard of care in the NHS).
- Staging: replacing surgery with endosonography as the first-line investigation for mediastinal lung cancer staging throughout the NHS, and changing NICE Guidelines.
Treatment: reducing side effects in breast cancer by giving partial breast radiotherapy to women with low-risk early stage cancer (NICE Guidelines changed).
Critical success factors
Critical success factors were:
- The appointment of Programme Managers to each programme (and in some cases, a part-time Communications Manager) was critical to organising the programmes, their collaborations, meetings, events, budgets, recruitments, and pump priming activities. The Programme Managers focus on process, enabling the programme members and Leads to focus on science and clinical excellence, and creating sustainability of the programmes and the centre – even through the Covid-19 epidemic.
- Having delegated budgets for each programme allows the programme to be more self-determining, rather than a top-down approach. This releases creativity within the programmes, and directs resources towards impactful investments.
- Regular reporting and accountability. Critical to this is the peer scrutiny and challenge of the strategy and outcomes within the Executive Committee and from the Centre Director.
- Incentivisation for growth. Programmes know that if their current activities maximise impact and attract more competitive funding, there is a possibility of forming virtual or physical institutes within the Centre structure.
- Inclusion of 34 University Departments, 8 Institutes (some outside the University (e.g. Wellcome Sanger)) 2 University Hospitals and industrial partners.
Next steps
Next steps include:
- Revision of the Programme Structure for 2022-27 to grow more programmes and institutes
- Quinquennial review of the present programmes by Cancer Research UK within the Major Centre Grant.
- Continued review and advice from the International Scientific Advisory Board.
- Building a Cancer Research Hospital to co-locate key scientific facilities with clinicians, triallists and patients to spur new innovations for patient benefit.